English
English
 Français
Français
") 中文 (中国)
中文 (中国)
 Español
Español
") Português (BR)
Português (BR)
An initial good clinical examination is necessary to assess the feasibility of each technique, which differs from one patient to another.
A reconstruction with prosthesis will be possible if the scar’s flexibility is satisfactory and the skin tissues thick enough after the mastectomy.

Soft skin tissues despite irradiation of the skin
The reconstruction with dorsal flap appears more or less simple depending on the quantity of tissue that can be withdrawn from the back without causing excessive tension.

Soft skin tissues without excessive tension
Reconstrution with TRAM flap requires a sufficient donor area.

TRAM flap possible even with a small abdominal volume
Lipofilling can only be done in accordance with liposuction possibilities.

Enough fat in the thigh area for two Lipofillings after tram flap
Once the possibilities have been evaluated, the choice may be limited, due to the patient’s morphology and mostly to prior radiotherapy. When there was no radiotherapy, a reconstruction with prosthesis is often possible, even in situations that seem complicated.

From Left to Right :
Unsightly mastectomy scar
Bilateral reconstruction satisfactory with prosthesis
After radiotherapy, reconstruction with prosthesis is more difficult, if not impossible. In that case, a reconstruction with autologous skin flap is indicated.
From Left to Right :
Right side irradiated Bad result after dorsal flap on the right
Reconstruction with TRAM flap on both breasts
When several options are possible, the patient has the ultimate choice, after having been notified of the consequences of each reconstruction technique.
Recontruction with TRAM flap uses the skin and fat excess of the lower umbilical abdominal area, often existing with women over 40 years-old, who may find satisfaction in an associated tummy tuck. This reconstruction has the disadvantage of requiring a recovery of 6 weeks after the operation. However, it is definite and stable over time, as the obtained symmetry will remain the same, regardless of the patient’s weight evolution.
The post-operative pain often feared by patients is actually quite bearable in most cases. In the first few days following the surgery, appropriate analgesics are given and patients can leave the clinic after 5 to 7 days of hospitalization. A complete rest of 15 days is required after returning home before gradually resuming a normal activity.
Returning to work, possible after 6 weeks for an office job, is adjusted depending on each situation. A tension of the abdominal wall is felt during the first weeks, especially if the abdominal excess was limited. It starts to fade and disappear within a few months. The resumption of sport practice is possible after 3 months. There are no contraindications later on besides carrying very heavy loads.
Reconstruction with prosthesis is not as heavy but usually requires 2 operations, with a few days’ hopitalization and 3 to 4 weeks recovery. It is easy to realize in immediate breast reconstruction and suitable with adjuvant chemotherapy. However, the patient should be warned that the result doesn’t always look natural and there is a high risk of asymmetry after a few years (causing re-operations).
Reconstruction with dorsal flap requires a few days’ hospitalization. Recovery is in general quite fast, from 4 to 6 weeks. The current trend is to make more and more inconspicuous scars, in particular for immediate autologous reconstructions. There is a risk of seroma usually resolved after a few punctures, and much more rarely fibrosis on the sample area which may cause functional disability and afterpains that go away within a few months.
The patient’s decision, in addition to these elements and her age, will depend on other factors such as her family and career situations, which might lead her to choose a reconstruction that doesn’t involve extended unavailability.
For athletic patients, or those having a job requiring physical activity, a reconstruction with prosthesis is to be indicated, avoiding the use of a muscle and skin flap that could lower their physical abilities.
In the end, the patient’s wish and what she really wants must be respected as much as possible in order to help her deal better with the psychological disadvantages of each technique. A momentary discomfort after a desired reconstruction (with prosthesis or with flap) can turn into an unbearable pain for a patient that underwent, rather than chose, the same surgery.
When in doubt, it is better to offer the simpler reconstruction with prosthesis. In fact, a correction using an autologous skin flap is often possible later on, if the patient is not satisfied.

From Left to Right :
Bad result with expander
Resection of prosthesis TRAM flap

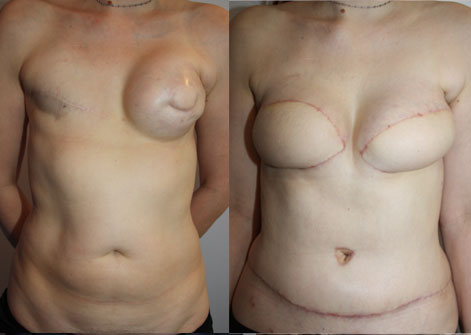
From Left to Right : :
Capsula contracture after prosthesis reconstruction
Correction with TRAM flap
Other Articles