English
English
 Français
Français
") 中文 (中国)
中文 (中国)
 Español
Español
") Português (BR)
Português (BR)
This is a technique I have extensive experience of (with over 600 TRAMs carried out since 1989), and for which I have set up a procedure making it very reliable, reducing to 1% the risk of partial flap necrosis.
The TRAM is a flap using one of the two rectal muscles from the abdominal wall, sectioned on its lower part, in which circulate epigastric vessels that allow blood circulation in the fat and skin flap.
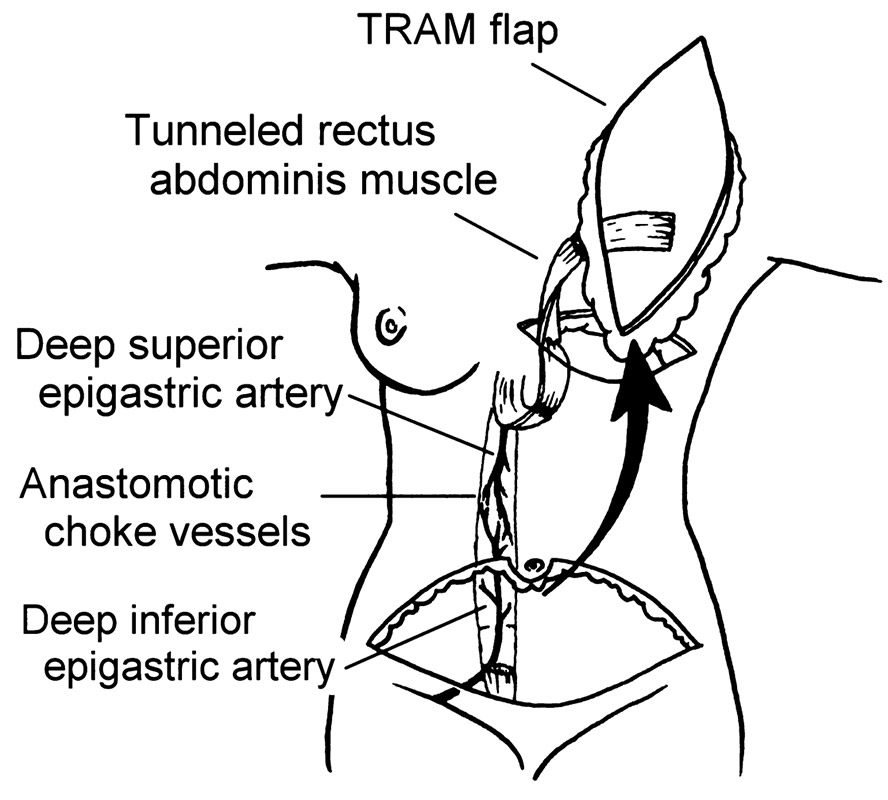
La vascularisation du TRAM
Superior and inferior epigastric vessels all meet in the rectus abdominal muscle.
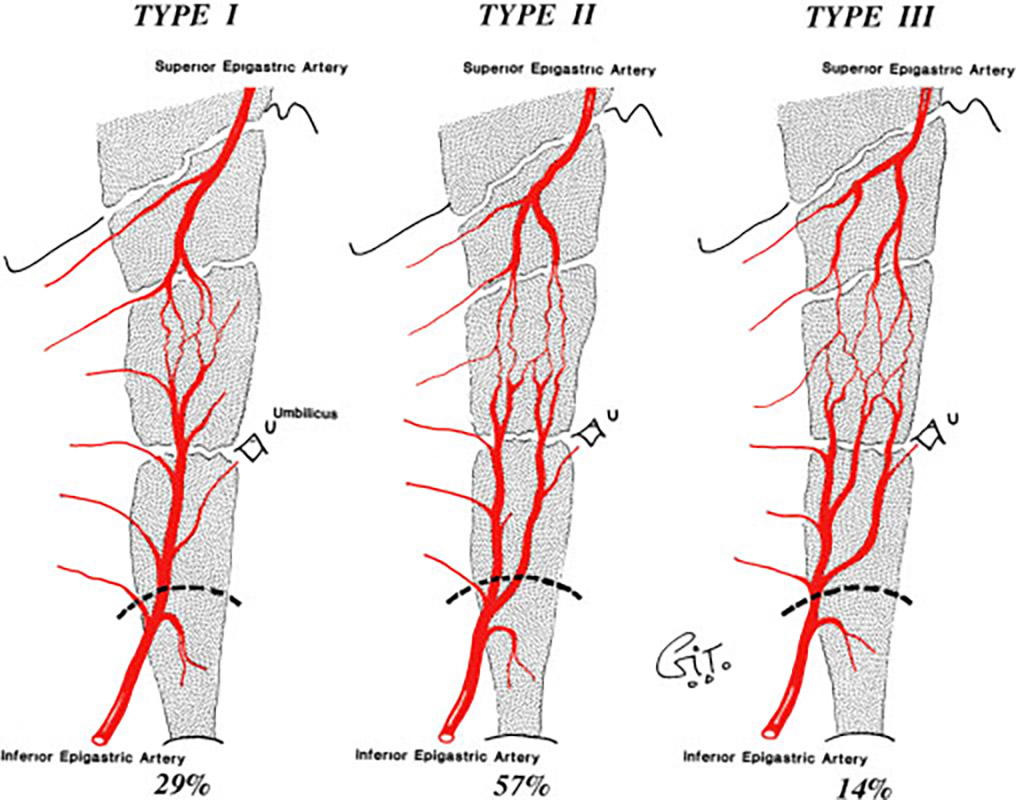
Upper and Lower Episgatriscal vascularization anastomoses in the rectal muscle
Before preparation, inferior epigastric vascular flow is predominant.
 Angioscanner avant préparation |
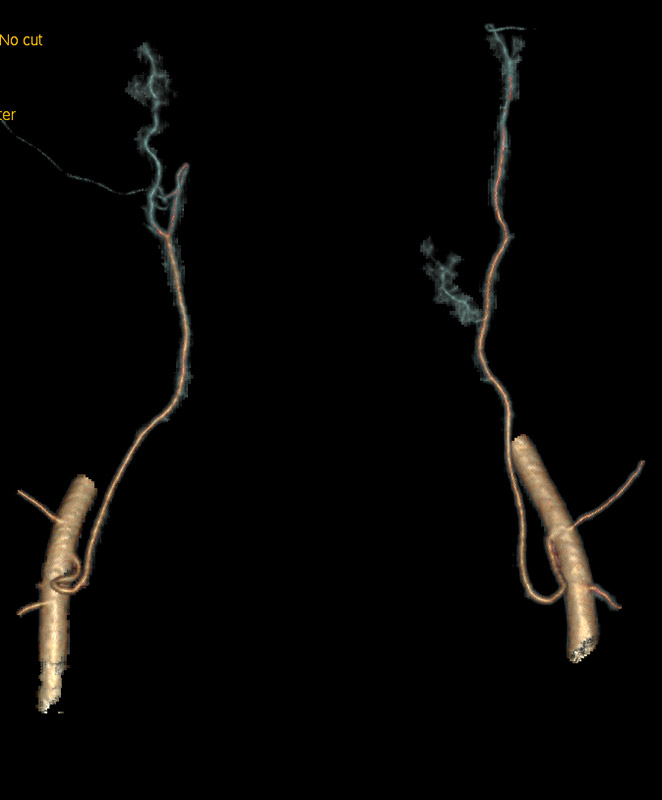 Flux épigastrique venant du bas |
To improve vascular blood flow (and thus reduce the risk of a poor vascularization and a subsequent flap necrosis) a preparation has to be done beforehand. It consists in a ligation of the inferior epigastric vessels, which reverts the impulse of the vascular blood flow and permits the resumption of vascularization for inferior epigastric vessels
 Angioscanner après préparation |
 Flux épigastrique venant du haut |
It can be done through surgery (sometimes in the same time as the mastectomy, if this reconstruction is planned from the start) or through embolization (at the vascular radiology department of the Clinique de l’Orangerie, under local anesthesia).
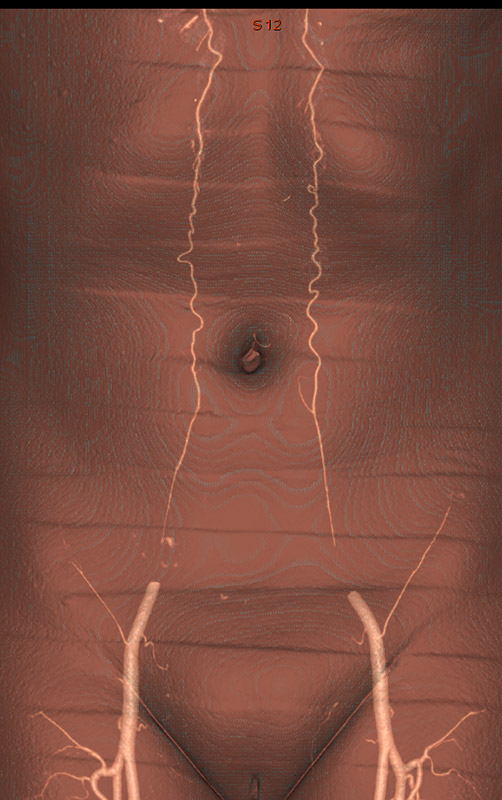
The angiography scan made subsequently shows the quality of the superior epigastric vascularization,
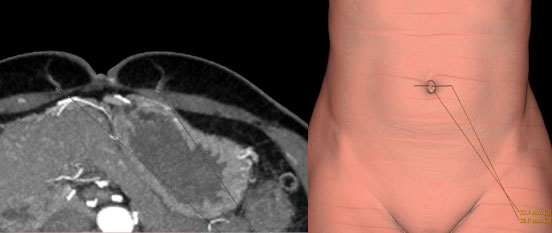
Visualization and localization of perforator vessels
and makes sure that it is sufficient for a good flap vascularization. If this vascularization is asymmetrical, the angiography scan allows to choose the best side.

asymmetric vascularization left side with better quality
The muscle removal creates a weakness in the abdominal wall that patients cannot feel in their daily life. The risk of loosening of the abdominal wall or incisional hernia is prevented during the operation with the introduction of a synthetic mesh to support the abdominal wall when it looks fragile. This non-absorbable mesh will be totally unnoticeable for the patient later on. In my pratice, 60% of patients had mesh placed during the reconstruction, 2% had a parietal complication or post-operative incisional hernia, and only half of them (1%) had to be reoperated for it.
Reconstruction with TRAM gives a very natural result with an associated tummy tuck.

From Left to Right :
Before right breast mastectomy
After right breast reconstruction with TRAM flap and opposite breast symmetrization
It is not suitable for patients with arterial vascular risk (angiopathy or Raynaud’s syndrome), or veinous thrombosis (related to an abnormal V Leiden factor). Due to a higher risk factor related to smoking and obesity, I only offer this technique for non-smoking patients or those having fully quit for at least 6 months, with a body mass index under 30. Age also being a risk factor, all patients over 60 years old should be in great shape.

From Left to Right :
67 years-old patient with suitable body shape and
very healthy
Result after operation
This surgery can sometimes result in a very benificial makeover for the patient.

From Left to Right :
Sufficient abdomen and
opposite breast hypertrophy
Result after tram flap and opposite breast reduction
It can be suitable even when the abdomen seems to lack volume and the body mass index is under 20.

From Left to Right :
Patient with a 19 BMI
final result over time
It can be resorted to even in case of median scar under the navel, then using only half the tissues under the navel.

From Left to Right :
Lower Abdominal scar
half TRAM Reconstruction
In some situations (immediate reconstruction, or a patient who doesn’t tolerate a reconstruction with prosthesis), a TRAM can be done de-epitheliazed to limit scarring.

From Left to Right :
Reconstruction with expander
And TRAM flap
More seldom can TRAM be done on both breasts, as it brings in more risks to the abdominal wall.

From Left to Right :
Important radiotherapy sequels
Secondary reconstruction with a bilateral TRAM flap
Other techniques